

ThitareeSarmkasat/iStock via Getty Images
In a somewhat circuitous fashion, I will attempt to explain why some Alzheimer’s drug candidates are more likely to be successful than others.
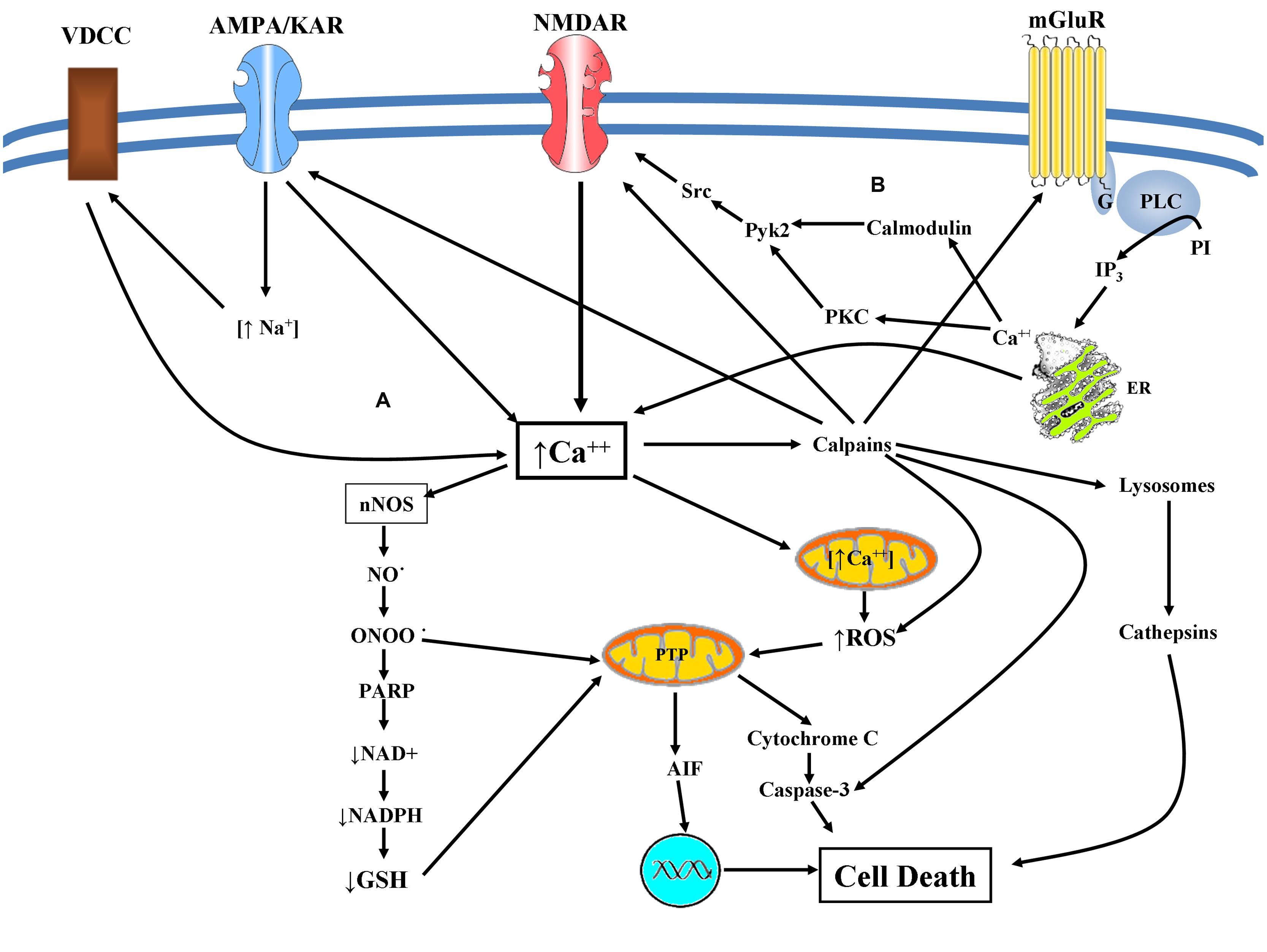
Predominantly two receptor types are involved in the development of Alzheimer’s disease: g protein-coupled receptors and receptor tyrosine kinases. The over-activation of either of these receptor types can lead to either cell growth via the phosphatidylinositol-3 kinase/Akt pathway or cell death via sustained production of oxidants and caspase-3 activation. These signaling pathways are like a dual valve. When they are turned on together, they help maintain health. But when one is shut off or the other cannot be turned off, a series of diseases ensue. In the case of Alzheimer’s disease and some other neurological diseases, the nitration of phosphatidylinositol 3-kinase leads to cell death without cell growth. In some types of cancer, the oxidation of PTEN (phosphatase and tensin homolog) prevents the dephosphorylation of the phoshatidylinositol 3,4,5 triphosphate which leads to cell growth without cell death. Interestingly, the same factors can lead to both oxidation and nitration, so it is largely a matter of which affects the phosphatidylinositol 3-kinase/Akt pathway first. To put it another way, the same triggers that can lead to some types of cancer can also lead to Alzheimer’s disease and other neurological diseases. However, they usually do not lead to both (studies).
{kind=link}
If the above analysis is correct than the treatment of Alzheimer’s disease would appear simple, either increase the activation of the phosphatidylinositol 3-kinase or decrease the activation of the pathway that leads to the sustained production of oxidants and caspase-3 activation. But neither approach has worked well in Alzheimer’s disease. The use of various growth factors (also known as trophic factors) to activate the neuroprotective phosphatidylinositol 3-kinase/Akt pathway has not been successful to date. This includes insulin, brain derived neurotrophic factor, and nerve growth factor. It will likely include Athira’s (ATHA) efforts to enhance the activity of hepatocyte growth factor. Synaptogenix’s (SNPX) (formerly Neurotrope) byrostatin-1 by activating protein kinase C, and then NMDA receptors, and calcium influx (chart in article) increases expression of brain derived neurotrophic factor, but has produced muddled results. The problem is that growth factors are largely ineffective in the treatment of Alzheimer’s disease because the pathway through which they operate is largely blocked by nitration.
The following quote is for ALS, but it likely also applies to Alzheimer’s disease:
Oxidative stress mediated by nitric oxide (NO) and its toxic metabolite peroxynitrite has previously been associated with motor neuron degeneration in amyotrophic lateral sclerosis (ALS)…Motor neuron death was largely prevented by NOS [nitric oxide synthase] inhibitors and peroxynitrite scavengers but not by trophic factors that otherwise will support motor neuron survival in the absence of astrocytes (source of quote).
Riluzole – a protein kinase C inhibitor – which inhibits protein kinase C activity and the subsequent formation of peroxynitrite is an example of a drug that should reduce cell death in various neurological diseases. However, riluzole has only a limited effect on ALS and in the case of Biohaven’s (BHVN) pro-drug failed in the treatment of Alzheimer’s disease (results). The following likely explains why:
Finally, riluzole inefficacy against ntirosative stress might support the idea that a combined therapeutic intervention may results more effective in ALS patients, as in the case of co-administration of edaravone, a drug known to reduce RNS [reactive nitrogen species]. (source of quote)
What is probably true for ALS is also likely true for Alzheimer’s disease: drugs and drug candidates that slow down the production of oxidants at best only slow down the progression of Alzheimer’s disease. In the case of anti-amyloid drugs/drug candidates such as Biogen’s (BIIB) Aduhelm, Biogen and Eisai’s (OTCPK:ESALY) lecanemab (BAN2401), and Alzheon’s ALZ-801 (tramiprosate) only APOE4 carriers see any very modest reduction in the progression of the disease. Eli Lilly has not yet broken down its numbers for donanemab based on APOE4 status, but its overall numbers are similar to Aduhelm (donanemab versus Aduhelm/aducanumab, p. 9). FDA approval for donanemab is not guaranteed and even if approved, Medicare will look at the numbers very carefully to see if it deserves general coverage. The most likely outcome is that Eli Lilly will end up in a similar place as Biogen.
The removal of amyloid makes a minor difference for APOE4 carriers since they have higher levels of amyloid and oxidative stress to begin with (amyloid is in part the product of oxidative stress and then can add to that stress). The two advantages of ALZ-801 over the others is that by blocking amyloid production rather than removing amyloid it does not produce brain swelling or brain bleeds and it is given orally rather than intravenously.
While the evidence is not air tight, it seems that the key to treating Alzheimer’s disease and a number of other neurodegenerative disease is to not only slow down the production of oxidants, but to scavenge them, and to reverse part of the already existing damage that they have done to the brain.
Aricept, Anavex’s (AVXL) blarcamesine, and perhaps Cassava Sciences’ (SAVA) simufilam inhibit the formation of peroxynitrite by limiting the release of intracellular calcium. Aricept by increasing hydroxybutyrate levels (a ketone body) and simufilam due to its ketone functional group accelerates the decomposition of peroxynitrite which helps stabilize Alzheimer’s disease for at least a year, with simufilam producing better results at one year than Aricept. Blarcamesine – a tetrahydrofuran derivative – may directly scavenge peroxynitrite. Panax ginseng inhibits the formation of peroxynitrite by limiting the activation of Nuclear factor kappa B and scavenges peroxynitrite. Cyclo Therapeutics (CYTH) a cyclodextrin/polysacharide derivative by removing cholesterol limits the size of lipid rafts in which the processes that lead to neurodegeneration (and perhaps cancer) occur and scavenges peroxynitrite. Blarcamesine – a tetrahydrofuran derivative – may also scavenge peroxynitrite. Trappsol Cyclo led to improvements in one Alzheimer’s patient that were sustained for a year and a half (case study). Panax ginseng leads to improvements in cognition that were sustained for at least two years (trial results). Blarcamesine came close to stabilizing Alzheimer’s disease for three years (graph, p. 17). Cyclo Therapeutics has begun a phase 2 clinical trial for Alzheimer’s disease, the results of which will be key for the company whose current stock value is under 3. Trappsol Cyclo and blarcamesine may represent the best hope in terms of drug candidates for treating Alzheimer’s disease at this point and in the long-term Anavex and Trappsol may represent the best investment opportunities. The results from a phase 2b/3 clinical trial for blarcamesine due later this or early next year may be pivotal in the history of Alzheimer’s disease treatment.
It is difficult if not impossible to regenerate neurons in the hippocampus without first reversing nitration. And one can only slow cell death by slowing down the production of oxidants rather than removing them. At this point very few drugs being studied for the treatment of Alzheimer’s disease do all three. The route to largely stabilizing the disease is becoming clearer even though the road to curing the disease has not. Slightly slowing the progression of the disease does little good, but achieving only incremental progression would be a godsend.
Be the first to comment