

XH4D/E+ via Getty Images
With anti-amyloid and anti-tau drugs not producing any breakthrough results for Alzheimer’s disease, treatments that modulate inflammation appear to be positioning themselves as the next major line of attack against the disease. Several companies – some of which are listed below – are working on drugs that reduce neuroinflammation and/or increase beneficial immune responses to remove amyloid and other “cellular debris”.
Leading Immune Modulating Drug Candidates for Alzheimer’s Disease
INmune Bio’s (INMB) XPro1595
Coya Therapeutics’ (COYA) COYA302
Alector’s (ALEC) AL101
For reasons to be discussed below, it is doubtful that any of these treatments will be successful against Alzheimer’s disease.
It is well-recognized that neuroinflammation contributes to oxidative and nitrosative stress in Alzheimer’s disease. What is less recognized is that the main source of neuroinflammation in Alzheimer’s disease is oxidative and nitrosative stress. Reactive oxygen species (such as hydrogen peroxide early in Alzheimer’s disease) and reactive nitrogen species (such as peroxynitrite) damage proteins and lipids (Damaged Associated Molecular Patterns) provoking an inflammatory response (via Toll-Like Receptors and Pattern Recognition Receptors). The following chart demonstrates this well:
Oxidation and Inflammation (Redox Biology)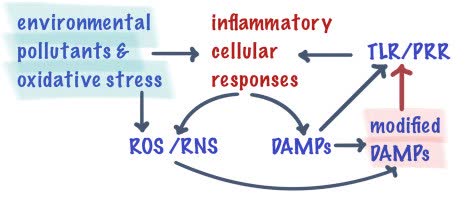
All factors which increase oxidative stress in the brain (environmental pollutants, a diet high in sugar and other carbohydrates, saturated fats, salt, high fructose corn syrup, and processed meats, psychological stress, heavy chronic smoking and drinking, traumatic brain injuries, chronic infections, misfolded amyloid and tau proteins, the APOE4 gene, various genetic mutations, and more) increase the risk for Alzheimer’s disease.
One can try to control nitro-oxidative stress immediately upstream of peroxynitrite formation (p38 Mitogen-Activated Protein Kinase, Nuclear Factor kappa B, Nicotinamide Adenine Dinucleotide Phosphate Oxidase, or inducible Nitric Oxide Synthase inhibition). In theory at least, this should be more effective than working downstream of peroxynitrite formation (i.e. via direct anti-inflammatories). Few of the many drug candidates that operate in this fashion, though, have reached late stage clinical trials (review article).
BioVie’s (BIVI) NE-3107 – an ERK (extracellular regulatory kinase) and Nuclear Factor kappa B inhibitor – came closest in this regards, but the placebo group, some of whom were on Namenda performed better than expected. There may be only a slight advantage by combining a NMDA receptor antagonist with compounds that act downstream of NMDA receptor activation, such as ERK, p38 MAPK, NFkB, NADPH oxidase, or iNOS inhibitors.
The key is not only to slow down peroxynitrite formation, but to scavenge peroxynitrite and to repair part of the damage that oxidation and nitration do to critical enzymes, transport systems, and receptors in the brain including those responsible for the synthesis of acetylcholine – the neurotrasmitter needed for the retrieval of short-term memory. Panax ginseng contains compounds such as saponins/ginsenosides that inhibit phospholipase C (which is overactive during the early stages of Alzheimer’s disease) and Nuclear Factor kappa B and also scavenge peroxynitrite. By doing so, panax ginseng leads to initial improvements in mild Alzheimer’s disease patients that are maintained for at least two years (clinical trial, figure two). Eugenol in various essential oils via aromatherapy also inhibits phospholipase C and Nuclear Factor kappa B and scavenges peroxynitrite, but only short-term data is available (clinical trial one, clinical trial two). By reducing oxidative and nitrosative stress, these treatments result in better neurotransmissions (due to the de-nitration/untangling of tau protein), increased blood flow in the brain, improvements in certain forms of memory and cognition (better sense of time and place, better recognition of people and objects, more awareness and alertness), some regeneration of neurons in the hippocampus, and less death of neurons
For moderate Alzheimer’s disease, where more extensive oxidative damage is done to parts of the brain that are not as amenable to repair (the frontal cortex versus the hippocampus), this approach can slow down the progression of the disease for at least a year (example, figure one).
While there are several anti-oxidant natural products that have shown promise in the treatment of Alzheimer’s disease, there are very few direct anti-oxidant drugs being tested for Alzheimer’s disease. Anavex (AVXL) 2-73/blarcamesine – a tetrahydrofuran derivative – is the only one that I know of that has completed a phase 2b/3 clinical trial. However, the results were obfuscated due to the combination of the 30mg and 50mg dose. At the higher dose, a considerable number of individuals experienced dizziness and/or confusion, which led either to down titration or dropouts. In those with a functioning sigma-1 receptor, Anavex inhibits intracellular calcium release (which limits oxidative stress early in Alzheimer’s disease). It may also scavenge hydrogen peroxide and peroxynitrite (through the donation of hydrogen atoms and electrons). At high concentrations (in a previous trial) and in certain individuals, blarcamesine appears to have nearly stabilized mild cognitive impairment and mild Alzheimer’s disease for three years. A much larger extension trial to be completed this summer will indicate if the results are real.
In Alzheimer’s disease, the brain’s main antioxidant – glutathione – is depleted, which leads to the oxidation and nitration/disabling of critical receptors, enzymes, and transport systems in the brain needed for proper brain function. Unfortunately, glutathione does not enter into brain cells well, which means that other antioxidants have to be used to treat the disease. Panax ginseng has an advantage in that it contains multiple antioxidant compounds and aromatherapy has the advantage that the antioxidant compound eugenol can almost directly be inhaled into the hippocampus. Whether there are natural products that are more effective against Alzheimer’s disease remains to be seen. And with the partial exception of Anavex’s blarcamesine, large-scale results for anti-oxidant drugs are a long ways away. The takeaway for investors is that for the time being, most Alzheimer’s drugs are going to continue to produce only middling results at best.
Editor’s Note: This article covers one or more microcap stocks. Please be aware of the risks associated with these stocks.
Be the first to comment